The Memorable Work of Medical Missions →
This blog is in progress.
For the past several years –nearly two decades– I have participated as a photographer in many medical missions. This mission work was done for different organizations, each specializing in different aspects of medicine. Many, though not all, these missions were conducted by one surgeon for a specific organization such as Smile Train, whose focus was on cleft lip and palate surgeries. The duration of most of these missions was about 7-10 days. My duties were to manage the database for these missions by taking photographs of the screening, surgeries and post operative photographs. In addition, I would document the overall mission and produce either a small film or a slide presentation for the mission. I would set up charts outside of each operating room, with each patient’s name and I’d track their surgical status, ensuring that each patient was photographed appropriately. For the cleft lip and palate patients, I would use a Dingman Retractor (an oral surigal devise used to retain the mouth for cleft palate and intraoral surgeries), a dental mirror and a ring light on my camera lens. Once all of the ‘before’ shots for each patient in the operating rooms had been completed, I would let the nurses know where I was and I’d usually do some portrait work nearby the hospital. I would gage the approximate time that it would take for the shortest surgery to be completed and make sure I was back in time for the post-op shots for each patient. Depending on the hospital or clinic that we were working, and the number of beds in each operating room, part of the mission’s goal was to do as many surgeries as possible each day. The missions I was involved with were mostly in South America and Southeast Asia though I also went to Uganda twice for mission work.
For me, each mission was an extraordinary experience. I loved the travel aspect of these missions but I also really enjoyed being fully immersed by the team of healthcare workers. I was keenly aware of the collaborative aspect of American doctors and nurses working alongside native doctors and nurses. Without idealizing the situation too much, most of these missions were learning experiences for all involved. That said, I was most impressed by how the medical teams were so hyper sensitive to the notion of colonialism. Though the goal was to teach the medical staff at the local hospitals, American and other visiting healthcare workers were tuned in to the fact that we were on someone else’s turf. Aside from being cordial, part of the mission was to join forces with the local staff and to become friends with them. A translator was usually present to assist with language barriers. Local doctors and nurses would be able to improve on their surgeries and offer the appropriate follow through care. Of course, many of the medical mission destinations, had staff that had been highly educated and who were highly skilled and so there was a give and take in much of the learning.
As a photographer, I was very aware that in America, I would not have had the opportunity to be in the operating room. During these missions, I experienced the full process of surgical operations. I felt so intensely for so many of the patients and their families and tried to capture some of the emotions that I witnessed which were all around me.

While on a Bolivian mission, led by Dr Arturo Batista, based in Texas, I was struck by the fact that Dr Batista was originally from Bolivia and that he wanted to go back to his home town and to help the local villagers who were very poor and would otherwise be without care. The medical mission took place in a local hospital but I made a few visits to Arturo’s local village. The villager’s showed me their clinic, their school and they cooked a meal for those of us who had made the visit.





Below is a photograph of the doctors engaging with the children and one of me ‘being a photographer!’ In the moments in between surgical photographs, I was interviewing Bolivan women for my ‘grandmother’s’ project. I set up my cameras to photograph both still and film footage of these women. I’d ask a series of questions that pivoted around their experiences with birthing, healthcare, survival and happiness. What I wasn’t able to communicate in espaniol, an interpreter would.






This is one of the grandmothers whom I photographed, interviewed and filmed for my ‘grandmother’s project.’
In Honduras, which I visited about four or five times, each for a medical mission led by Grant Thompson, MD, for his own mission, called Hand Help. Grant was a plastic surgeon based in New Haven, at Yale. I remember well, the burn patients and the snake bites. Hands were constricted and the goal of many of these hand surgeries was to bring some function back to the patient’s hands. Among so many of the patients, there was one little girl who took to me and I to her. We stayed in touch for years afterwards and when I’d come down to Honduras, I’d meet her at the hospital.



In Columbia, 2007, parents wait for their children to be screened.



I’ve been to Vietnam twice. My first trip was as participant to a mission in norther Vietnam, in Nagh Trong and the second time was a few years later, also as participant on a mission, in Cao Lanh which is on the left bank of the Mekong River, slightly south of Ho Chi Minh City (formerly Saigon). The city is a rice trading center, has a hospital and is linked by a road on the border of Cambodia.

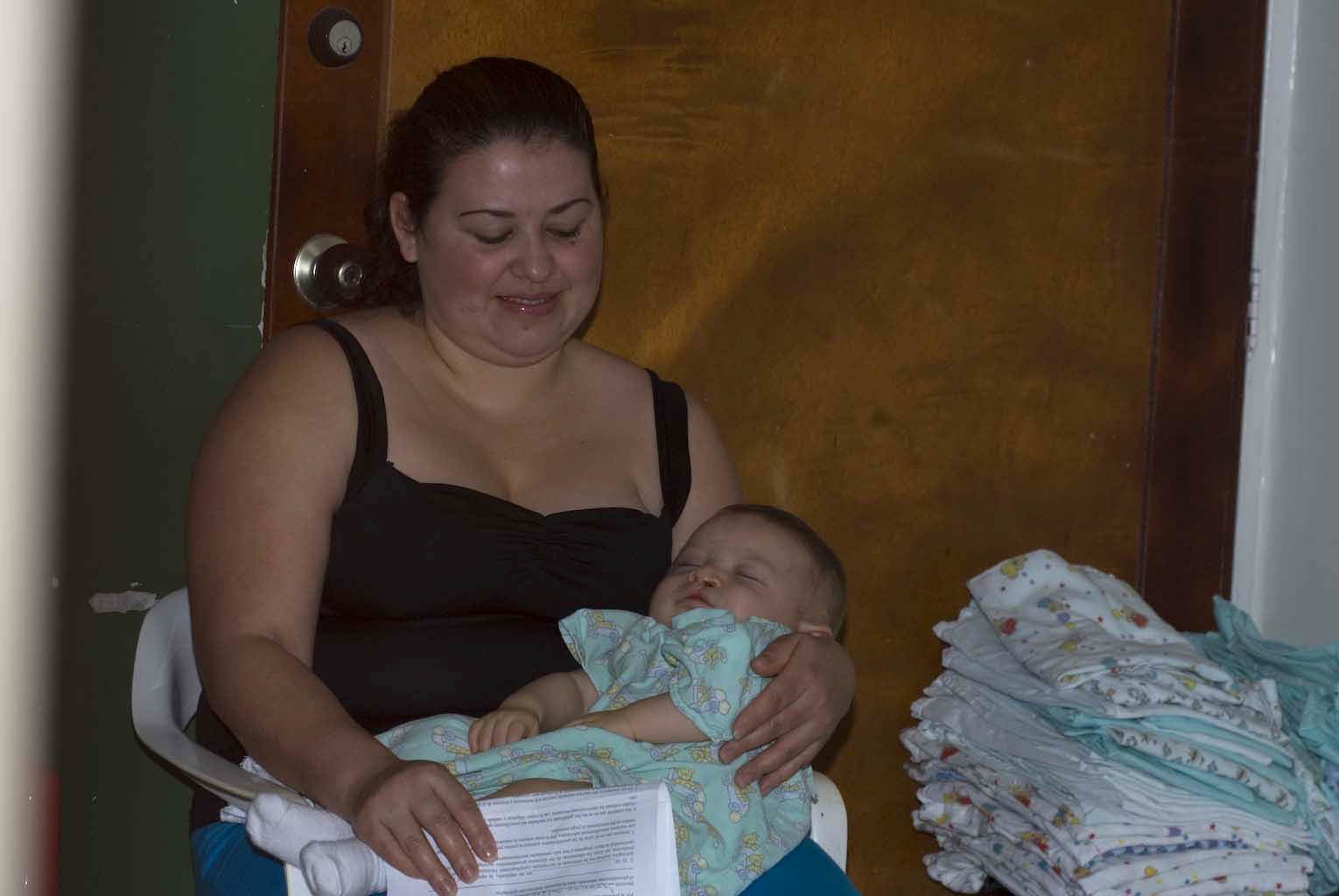
A mother pitches camp in a quiet corner of the hospital where her baby is scheduled to have her cleft lip and palate surgery the next day.




Thailand was a particularly memorable medical mission for so many reasons. The people are beautiful, generous with their smiles and their gratitude.